
8.09.2023
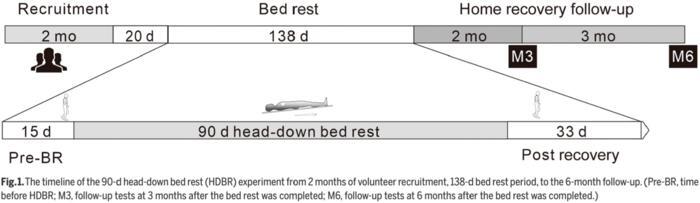
image: Fig. 1 The timeline of the 90-d head-down bed rest (HDBR) experiment from 2 months of volunteer recruitment.
When astronauts enter the space, they are exposed to weightlessness. Physiological and psychological challenges are waiting ahead. They may have a puffy face and experience space motion sickness, cardiovascular deconditioning, muscle atrophy, and bone loss. Moreover, long-term spaceflight has been shown to result in 83% of astronauts with postflight orthostatic intolerance. For above problems, exercise countermeasures can be the primary approach to resolve these changes. Head-down bed rest (HDBR) simulates physiological effects in weightlessness and is widely used in countermeasure testing, and efficacy of exercise interventions has been widely studied in HDBR with different periods as well. Usually, the long-term bed rest experiment is completed in stages, and a positive control of separated exercise countermeasures rarely tests at the same time in these experiments. In 2019, the Astronaut Center of China (ACC) held a 90-d HDBR in Shenzhen, Guangdong Province, China, which was planned as a whole and completed in 1 year. A separate treadmill running group and a resistance exercise group were designed as kinds of positive control. This HDBR was the first Chinese long-term spaceflight analog experiment. In a research paper recently published in Space: Science & Technology, authors from State Key Laboratory of Space Medicine Fundamentals and Application, China Astronaut Research and Training Center, Beijing, China, outline this 90-d HDBR and reports plain results reflecting the effects of exercise countermeasures.
First, authors introduce materials and methods used in the 90-d HDBR experiment. Experimental subjects are thirty-six healthy males (age: 32.0 ± 2.6 years; height: 167.7 ± 1.7 cm; weight: 63.4 ± 3.4 kg). They were randomly allocated to 1 of 5 experimental groups: a control group (CON; n = 8, HDBR without countermeasure), a RUN group (RUN; n = 7, HDBR with aerobic exercises), a RES group (RES; n = 7, HDBR with resistance exercises), a C1 group (C1; n = 7, HDBR with concurrent aerobic and lower-load resistance exercises), and a C2 group (C2; n = 7, HDBR with concurrent aerobic and high-load resistance exercises). All the subjects signed a written informed consent after a detailed explanation of the HDBR experiment. The ACC Ethics Committee approved this experiment, and the experiment was conducted under the accepted international rules and regulations. This experiment was divided into 3 periods: volunteer recruitment, HDBR period, and recovery follow-up, and was completed successfully in about a year (Fig. 1). The HDBR period consisted of 15-d adaptation and baseline measurements, a 90-d HDBR, and a 33-d recovery. During the bed rest period, subjects performed nearly all daily activities in the 6° head-down position and performed exercises in a supine position on a vertical treadmill, a head-down cycle ergometer, or a supine flywheel. Meanwhile, experimental state control, physiological & psychological support, and health condition monitoring were conducted. All data are presented as means ± SE. Descriptive statistics were used to calculate the subjects’ demographic. Two-way analysis of variance (ANOVA) statistics [group (5 factors) × time (2 factors)] with repeated measures was used to evaluate differences over time in each of the dependent variables. All statistical analyses were performed with SPSS 22.0 for Windows. The level of significance was set at P < 0.05.
Then, authors present the results of the experiment. Maximal aerobic fitness, peak workload, and HR are shown in Table 8. Significant interaction of group by time was detected for peak oxygen consumption. Moreover, the peak oxygen consumption and peak workloads were well upheld in the RUN, C1, and C2 groups after bed rest. All groups had similar peak HR before and after bed rest. As shown in Table 9, isometric muscle strengths increased after bed rest in the RES and C2 groups, which had performed flywheel resistive exercises. The squat MVC also improved 26.1 ± 11.6% and 20.5 ± 6.8% in the RES and C2 groups, respectively (Fig. 4B). However, in the CON group, there was 28.2 ± 3.0% decrease of squat MVC. No group differences existed for hip, femoral neck, or lumbar spine BMDs after the 90-d HDBR (Table 10). The hip BMD dropped from 1.73% to 3.80% in these 5 groups. In addition, there was no group by time interactions in the bone blood markers. However, the urine amino-terminal peptides were higher in the CON, RUN, and C2 groups than the C1 group (P < 0.048) (Table 11).
Finally, authors make draw the conclusion on this 90-d HDBR experiment. First, it is found running 30 min for 4 d a week can preserve the aerobic fitness after the 90-d HDBR. This result provides guidance for altering the time-consuming C1 group protocol. The change can save 29% of time, bring good compatibility, and keep the aerobic capacity and muscle strength. Second, the impact of exercise interventions on the bone needs to be evaluated in long-term spaceflight. It is recommended to consider about other causes on bone growth to keep bone health. In addition, the other causes may include pharmacological/nutrition-based interventions. Third, exercise prescription should consider about intraindividual variability to ensure safety and efficacy. Moreover, when prescribing and performing flywheel resistance exercises, special attention should be paid to the history of musculoskeletal disease. Fourth, in this experiment, the strong psychological support had a potential role in the physiological effects. In addition, the obscured bone health results meant a need for a strong nutrition provision. We should set up a compatible psychological support and nutritional provision to avoid excessive or inadequate support in a future long-term HDBR experiment.
Quelle: AAAS